
Oncology Client Work
In this project, I worked with the HCD team at RSM on a year-long client engagement with one of the largest networks of Oncology Centers in Texas. We were tasked with assessing the current state of patient and employee experiences with their telephony system, digital resources, and CRMs in order to propose the best strategic approach to the systems overhaul.
Over the course of this 1-year engagement, we conducted 2 rounds of research. First, we conducted 24 discovery interviews with stakeholders and employees, a stakeholder workshop, and a survey that received more than 200 responses from employees. Then, we went on-site for a week to conduct observational research at 6 clinics across the state, and a total of 43 intercept interviews with patients and patient caregivers.
I worked closely with 5 coworkers throughout this research engagement. In my role as a design researcher, I wrote interview scripts, lead interviews, did note-taking, wrote surveys, and worked with the team to synthesize research findings into key insights and future opportunities for each research deliverable to the client. The main systems used for this client engagement were Miro, Qualtrics, Figma and Microsoft.
Phase One
In our first round of research, we set out to define the problem through the lens of the stakeholder and employee experiences. In doing so, we gained a deep understanding of the inner-workings of the oncology network, and how it was supported by their technical systems.
Before conducting interviews, our team did preliminary research. This included competitive analysis research of other oncology networks, background research on problems that patients and operators might face in oncology, and research on the client to ensure we had an understanding of their jargon, their company structure, and their roles. This gave us a strong basis of understanding and helped us to brainstorm questions to ask in our interviews.
This phase of research was primarily reliant on insights gathered from interviews. We conducted 24, hour-long interviews with 10 Stakeholders, 3 Phone Operators, 4 Schedulers, 3 Triage Nurses, and 4 Physicians. All were conducted remotely via Webex. During these interviews, notes were taken in real time in spreadsheets, and then imported into Miro to be synthesized.

Synthesis
I took notes on 10 interviews, and was responsible for synthesizing the findings for each one. This synthesis was comprised of pulling key quotes and notes into the “What” column, writing a summarizing statement in the “So What” column, and then connecting them to a suggestion, idea, or question for further research in the “Now What” column.

After the first synthesis step, we had team meetings where those who lead each interview caught the rest of the team up on their synthesized findings. This ensured that the whole team had a full understanding of our findings that supported the rest of the synthesis process.
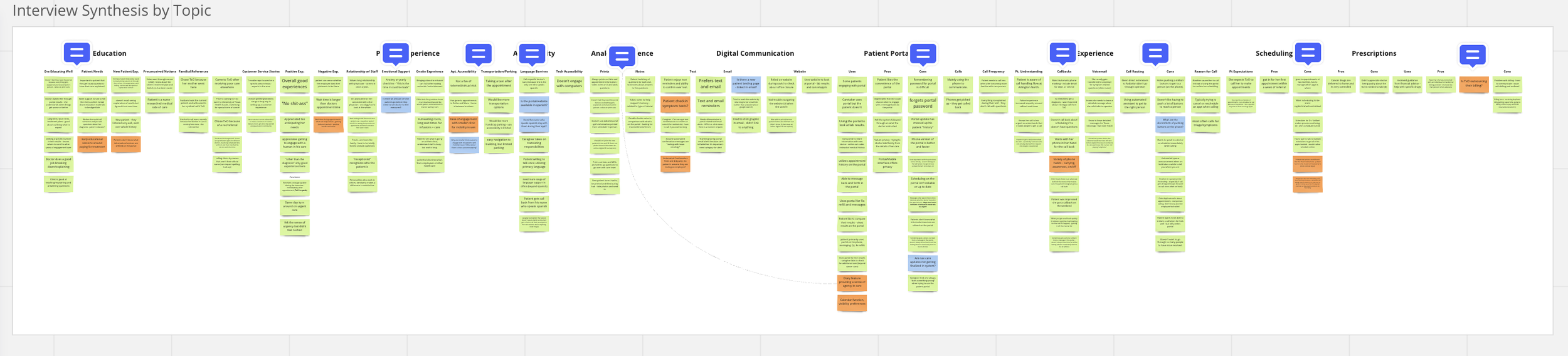
Following this step, we compiled the synthesized notes form every interview into one massive synthesis chart that worked to recognize patterns in our findings across each interview group.

For context, each tiny square has a quote, a key finding, or a future opportunity written on it.
In this chart, each column represented a topic, like ‘patient support touchpoints,’ or ‘reaching an operator,’ and each row was sorted by interview groups. Once our findings were sorted, we were able to write high level insight statements for each column. This method of synthesis allowed us to group findings in a way that visualized which points were reiterated the most, which had differing perspectives across roles, and acted as a basis for reference when sourcing interview quotes in our final research readout.
Using this research synthesis chart, we created a Research Readout slide deck that you can see here: Research Readout 1.
Phase Two
After delivering our first research readout, we identified the biggest gap in our understanding was in the patient experience. In order to understand the system needs on the front and back-end of the experience, it was crucial that we spoke to patients and patient caregivers to round out our findings and deliver the best strategic approach to the client.
Also, in our first round of research, we discovered issues within the employee network that impacted the effectiveness of the patient care flow. For example, there were problems with respect and communication, and the physical workspaces that impacted patient care. With both of these issues in mind, we made plans to go on site for a week to conduct observational research in a sample of oncology centers across the state of Texas, as well as intercept interviews with patients and patient caregivers.

On-Site Research
For one week, our team went on-site across the state of Texas. We visited 6 oncology centers, where we conducted observational research of the employee experience, and conducted 40 intercept interviews with patients and patient caregivers. While onsite, I switched between both roles; observational research and conducting interviews.
While observing, I asked employees questions about their experience, photographed workspaces, and noted problems I noticed. During this observational research, I found two things most interesting. First, understanding a place based on what you’re told pales in comparison to seeing it first hand. In person, I saw the layout of the oncology centers, the office spaces, the waiting rooms, the treatment spaces… It revealed a lot about the environment that impacted the day-to-day experiences of employees and patients. For example, Operators were often tucked away in tiny workspaces, shared offices were loud, and treatment spaces were cold with harsh lighting. Though these details are not directly related to a system, they impact the quality of work, the flow of communication between coworkers, and therefore the efficiency of patient care.
The second thing I noticed was how poorly the UI/UX of the systems were designed. It was shocking to see the user experience that employees thought was normal. For example, I watched one scheduler schedule 10 weeks of appointments for a patient. They were repeat appointments at the same time and same day every week. The scheduler needed to add each appointment and print a copy of the details, but there was no way to set an appointment on repeat. Every step took about 7 clicks in a slow-loading system, and every appointment required a different sheet be printed. The whole process took about 10 minutes with a sick patient standing there waiting.
It wasn’t that employees weren’t frustrated by the UX, they just lacked the ability to identify and communicate why the UX was so bad. Being there to observe allowed me to take notes on content structure, un-intuitive designs, color contrast, and redundancies that cluttered the user flow and made employees work less efficiently.

While onsite, I took most notes by hand, and transferred them online later.
Getting down direct quotes when writing on a clipboard was a huge challenge!
In addition to observational research, I conducted patient and patient caregiver intercept interviews. Our team conducted a total of 40 interviews while on site. We positioned ourselves in a private part of each oncology center, often in a conference room. Employees in the offices would direct patients to us to participate in interviews in exchange for a gift card. The process required interviewees to sign a participant waiver, and then lasted about 10-20 minutes. Using research from our first round of synthesis, We had developed an interview script ahead of our travel. This script asked rather basic questions. “Tell me about a time when you had to reschedule an appointment,” for example. The goal was to collect a large sampling of patient experiences with the phone system, scheduling, and the Oncology Network overall.
The most challenging part of these intercept interviews was gathering direct quotes in real time. Because of limitations to protect patient privacy, we could not record interviews. Also, our team was spread pretty thin. We were lucky that a lot of patients came for interviews, but this meant I was conducting and taking notes for them at the same time. Despite the challenge, I was able to jot down direct quotes from each interviewee that were important, and began to notice patterns in what they were saying.
Being on-site was a really exciting experience. The opportunity to get face-time with the client and employees was incredibly valuable. I got insight into the daily experiences of employees and patients that would have been lost in a remote research setting. We also got a great sampling of the diversity in oncology centers across the state. Se saw the good and the bad of the network, and came home with an incredible insight into the problem.
On-Site Synthesis

After our on-site research, my team and I began to synthesize all of our findings. First, we all had to transfer our written notes into Miro. Then the process was broken down into parts. We discussed our findings from patient and patient caregiver interviews first, then shared our observations of the employee experience. As we discussed all of our findings, we wrote key insight statements for both sets of research that were pulled into synthesis.
For this round of research, I took the lead on synthesizing our key takeaways. In order to see the patterns in our findings across all patients and locations, I sorted our key takeaways by topic. I grouped smaller topics, like experience with calling, patient expectations, and on-site experience into a larger flow of topics. This acted as a strong foundation for a research readout to the client.
I enjoyed structuring our key takeaways this way because it was a great way to visualize which topics came up most frequently across the board. For example, the patient portal came up a lot more than we expected. We learned that this digital resource had a lot of problems, but also presented a lot of opportunities for solutions.
Our research on site, especially with patients was crucial in our discovery process because we discovered problems and potential solutions outside of the call flow that had significant impact on the patient and employee experience. The value of UX research in the discovery phase of a project is to explore a problem from all sides, and learn how the user experience of an entire system impacts the problem at hand.
Check out the final research readout from our on-site research.